 We first met Louis, a now 6 ½ year old male Steppe eagle in June of 2024 when he had just been acquired as a potential mate for Amelia a 7 year old female.
We first met Louis, a now 6 ½ year old male Steppe eagle in June of 2024 when he had just been acquired as a potential mate for Amelia a 7 year old female.
 He had a history of an anklet injury to his left leg that resulted in a chronic wound to his left metatarso-phalangeal joint.
He had a history of an anklet injury to his left leg that resulted in a chronic wound to his left metatarso-phalangeal joint.
 Despite this the new owners took him on as they were happy to get it addressed themselves, which I have to say we fully supported as the plan was to remove all falconry equipment and put him into a breeding aviary. We all felt confident it would sort itself out…….how wrong we were!!
Despite this the new owners took him on as they were happy to get it addressed themselves, which I have to say we fully supported as the plan was to remove all falconry equipment and put him into a breeding aviary. We all felt confident it would sort itself out…….how wrong we were!!
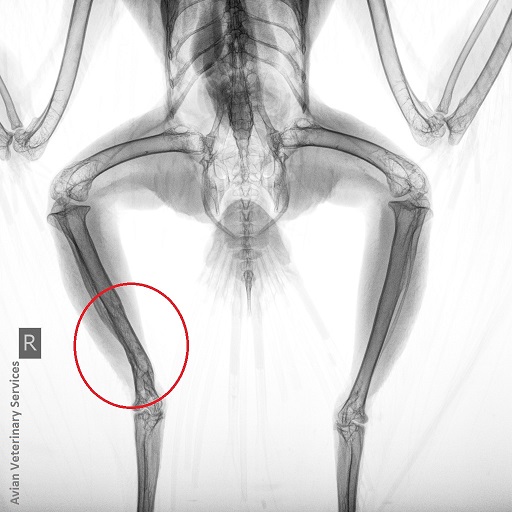
 At initial presentation the wound didn’t look too bad and X-rays revealed no obvious deeper structures/joint involvement e.g. arthritis. They did however show he had an old, healed fracture of his right tibiotarsus, but given the decent alignment and no obvious outward sign of lameness we felt was unrelated and of no real concern.
At initial presentation the wound didn’t look too bad and X-rays revealed no obvious deeper structures/joint involvement e.g. arthritis. They did however show he had an old, healed fracture of his right tibiotarsus, but given the decent alignment and no obvious outward sign of lameness we felt was unrelated and of no real concern.
 Under sedation we cleaned up and debrided the wound back to healthy tissue, dressed it and with covering antibiotics/anti-inflammatory medication and him now settled in his new aviary, we fully expected it to heal over the next few weeks.
Under sedation we cleaned up and debrided the wound back to healthy tissue, dressed it and with covering antibiotics/anti-inflammatory medication and him now settled in his new aviary, we fully expected it to heal over the next few weeks.
 Jump forward nearly a year and although the wound repeatedly got to roughly 80% healed, as soon as dressings were removed the central area, being right on the fold of skin above the hind toe, ‘refused’ to heal, would develop ‘proud tissue’ and regress to a scabby mess.
Jump forward nearly a year and although the wound repeatedly got to roughly 80% healed, as soon as dressings were removed the central area, being right on the fold of skin above the hind toe, ‘refused’ to heal, would develop ‘proud tissue’ and regress to a scabby mess.
 Throughout this Louis had been the model patient tolerating dressings fine, taking all his meds and, as eagles go, an absolute pleasure to deal with……he certainly deserved to get better, but sadly this was indeed starting to look like a potentially life-threatening situation!
Throughout this Louis had been the model patient tolerating dressings fine, taking all his meds and, as eagles go, an absolute pleasure to deal with……he certainly deserved to get better, but sadly this was indeed starting to look like a potentially life-threatening situation!

 At this point we turned to probably the world’s leading authority on such cases, retired avian specialist, Nigel Harcourt-Brown FRCVS author of the Birds of Prey – Anatomy, Radiology and Clinical Conditions of the Pelvic Limb, which I refer to on an almost weekly basis.
At this point we turned to probably the world’s leading authority on such cases, retired avian specialist, Nigel Harcourt-Brown FRCVS author of the Birds of Prey – Anatomy, Radiology and Clinical Conditions of the Pelvic Limb, which I refer to on an almost weekly basis.
 He pointed out that the affected area is actually the thickest area of skin of the whole avian integument and therefore would likely be the slowest to organise even if all was healthy, however from the images we shared he suspected we had a sequestrum of fibrous scar tissue that was not allowing normal granulation and epithelisation of the wound.
He pointed out that the affected area is actually the thickest area of skin of the whole avian integument and therefore would likely be the slowest to organise even if all was healthy, however from the images we shared he suspected we had a sequestrum of fibrous scar tissue that was not allowing normal granulation and epithelisation of the wound.
 We decided the only chance of moving forward was to excise this ‘non-healing’ area, but the problem we then had is that due to the non-elasticity of the scaly skin we would be unable to close the deficit without some form of skin graft. Also, the lesion was directly over of the lubricated tendon sheaths and extensor tendons of the hind toe that could easily be damaged during surgery in this area.
We decided the only chance of moving forward was to excise this ‘non-healing’ area, but the problem we then had is that due to the non-elasticity of the scaly skin we would be unable to close the deficit without some form of skin graft. Also, the lesion was directly over of the lubricated tendon sheaths and extensor tendons of the hind toe that could easily be damaged during surgery in this area.

 Under Nigel’s guidance, using cadavers kindly donated by our clients for exactly this purpose; to help other patients, we experimented with various ‘transpositional’ techniques where a strap of skin including its blood supply is moved from an area of ‘less tension’ to help cover the deficit. We eventually settled upon a rotational transposition flap as shown.
Under Nigel’s guidance, using cadavers kindly donated by our clients for exactly this purpose; to help other patients, we experimented with various ‘transpositional’ techniques where a strap of skin including its blood supply is moved from an area of ‘less tension’ to help cover the deficit. We eventually settled upon a rotational transposition flap as shown.

 The surgery, almost a year after he first presented to us, went as well as we could have hoped and to remove pressure, prevent flexion and protect the healing site a mouldable thermoplastic shoe was formed and applied.
The surgery, almost a year after he first presented to us, went as well as we could have hoped and to remove pressure, prevent flexion and protect the healing site a mouldable thermoplastic shoe was formed and applied.

As usual Louis didn’t bat an eyelid, he accepted the new footwear and continued to do exactly as we wished over the next 3 months, this involved weekly dressing changes which he got so used to it that he would just lie down to be picked up for. Part of the graft died-off, but the new blood supply clearly did its job and allowed full granulation/epithelisation, things improved week on week to the point now that the foot looks pretty normal again for the first time in, I suspect, over 2 years.
used to it that he would just lie down to be picked up for. Part of the graft died-off, but the new blood supply clearly did its job and allowed full granulation/epithelisation, things improved week on week to the point now that the foot looks pretty normal again for the first time in, I suspect, over 2 years.

 As well as Nigel, a special thanks goes out the team at Muncaster Hawk & Owl Centre for Louis’ ‘outpatient’ care and to Louis himself for being such a gentleman throughout his ordeal.
As well as Nigel, a special thanks goes out the team at Muncaster Hawk & Owl Centre for Louis’ ‘outpatient’ care and to Louis himself for being such a gentleman throughout his ordeal.

We are all really looking forward to little Louis flying about at some point 
 soon!
soon!